Increasing Treatment Adherence Through Digital Patient Engagement
Why chronic care needs support between visits
In chronic care, treatment success is rarely determined only during the clinic visit.
It is determined in the weeks and months between visits — when patients are at home, managing medication routines, lifestyle changes, side effects, treatment expectations, and uncertainty about what to do next.
For conditions such as obesity, diabetes, cardiovascular disease, respiratory disease, dermatology, oncology supportive care, and other long-term therapies, adherence and persistence remain major real-world challenges.
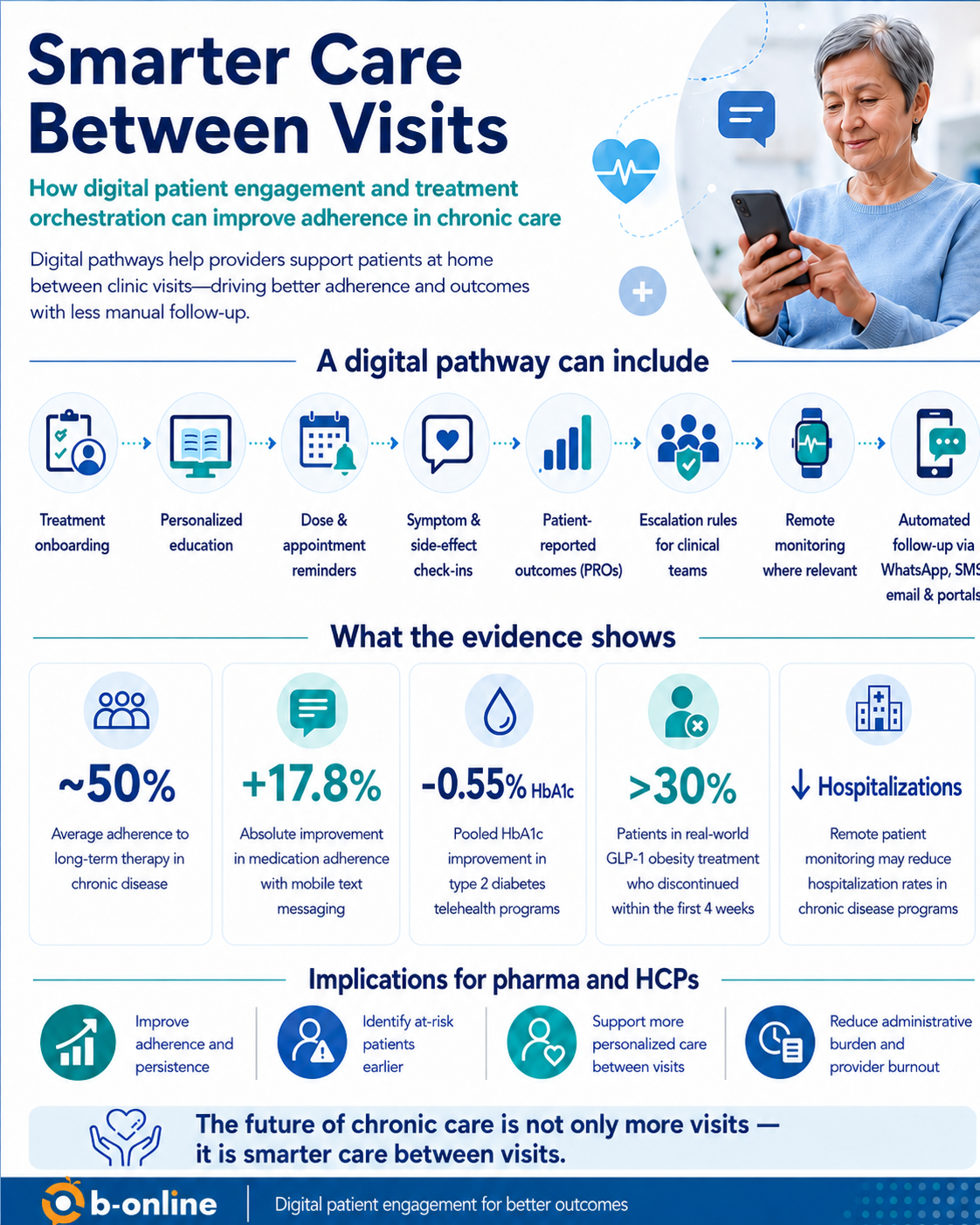
The World Health Organization has reported that adherence to long-term therapy for chronic diseases averages around 50% in developed countries. This means that even when effective treatments are available, a significant proportion of patients may not receive the full clinical benefit because they do not continue therapy as intended or do not follow treatment recommendations consistently.
This creates a clear challenge for healthcare systems, HCPs, and pharmaceutical companies:
How can we support patients between visits without adding more manual workload to already stretched clinical teams?
From reminders to treatment orchestration
Digital patient engagement should no longer be viewed only as a reminder system.
A medication reminder can be useful, but chronic care requires more than reminders. Patients often need structured guidance, education, monitoring, and timely escalation when something changes.
This is where digital treatment orchestration becomes important.
Treatment orchestration means using digital tools to guide patients through a predefined, personalized treatment pathway — based on their condition, treatment stage, risk factors, responses, and needs.
A well-designed digital pathway can include:
Treatment onboarding
Personalized patient education
Dose and appointment reminders
Symptom and side-effect check-ins
Patient-reported outcomes
Remote monitoring where relevant
Automated follow-up through WhatsApp, SMS, email, portals, or AI-supported assistants
Escalation rules for clinical teams when intervention is needed
The objective is not to replace the HCP.
The objective is to help the HCP identify which patients need attention, when they need it, and why.
The evidence behind digital engagement
There is growing evidence that digital interventions can support adherence and chronic disease management when they are designed around clinical workflows and patient behavior.
A JAMA Internal Medicine meta-analysis of 16 randomized clinical trials found that mobile phone text messaging approximately doubled the odds of medication adherence in chronic disease. In practical terms, the authors estimated that adherence could improve from an assumed baseline of 50% to 67.8% — an absolute improvement of 17.8 percentage points.
In type 2 diabetes, telehealth interventions have shown measurable clinical impact. A systematic review of systematic reviews found that telehealth interventions were associated with a pooled HbA1c improvement of approximately -0.55% compared with usual care.
In obesity management, smartphone app interventions have shown statistically significant reductions in body weight and BMI over 4–6 months. However, the evidence also shows that long-term sustainability is more difficult when digital interventions are not sufficiently personalized or do not provide continuous support.
This is particularly relevant for GLP-1 obesity treatment. Real-world analyses have shown that early discontinuation remains a challenge, with more than 30% of patients stopping treatment within the first four weeks in some datasets. Provider follow-up and specialist involvement were associated with better persistence.
Remote patient monitoring also appears promising across chronic disease programs. A 2025 systematic review found that remote monitoring may reduce the proportion of patients hospitalized, the number of hospitalizations, and hospital length of stay compared with usual care, although certainty varies by disease area and program design.
Together, these findings support a practical conclusion:
Digital engagement is most valuable when it is not isolated from the treatment pathway, but embedded into a structured model of care.
Why this matters for obesity and diabetes
Obesity and diabetes are strong examples of treatment areas where between-visit support is critical.
In obesity care, patients may need support with treatment initiation, dose escalation, expectations, nutrition, side-effect management, motivation, and long-term persistence. For GLP-1 therapies, early discontinuation may prevent patients from reaching therapeutic dose or achieving meaningful outcomes.
In diabetes care, patients may need support with medication adherence, glucose monitoring, lifestyle behaviors, risk-factor management, and understanding when to contact the care team.
In both areas, treatment success depends not only on the therapy itself, but also on the patient’s ability to stay engaged over time.
Digital pathways can help by delivering the right intervention at the right stage:
Before treatment starts: education and expectation setting
During initiation: onboarding and adherence support
During titration: side-effect check-ins and escalation rules
During maintenance: persistence support and behavioral reinforcement
Before visits: patient-reported outcomes and preparation
After visits: follow-up tasks, reminders, and next-step guidance
Supporting HCPs, not adding more work
One of the risks of digital health is creating more data, more dashboards, and more tasks for clinical teams.
This is why orchestration is different from simple digital communication.
A good digital pathway should filter, prioritize, and escalate. It should not require HCPs or nurses to manually review every patient interaction.
Instead, the system should help classify patient needs:
Patients who are progressing well continue through automated support.
Patients who miss steps receive automated reminders or education.
Patients who report concerning symptoms are escalated.
Patients at risk of discontinuation are flagged.
Patients who need clinical input are routed to the right team member.
This allows care teams to focus human attention where it has the highest clinical value.
Reducing provider burnout and administrative burden
Provider burnout is strongly associated with administrative workload, documentation burden, and inefficient digital systems.
Digital tools should therefore be designed to reduce low-value manual follow-up, not increase it.
When implemented correctly, digital patient engagement can help reduce repetitive administrative work by automating routine communication, collecting structured patient-reported information, preparing patients for visits, and identifying which patients require attention.
This is especially important in high-volume chronic care programs, where manual follow-up for every patient is often not scalable.
Implications for pharma and healthcare providers
For pharma companies and healthcare providers, patient engagement should not be treated as a separate “nice-to-have” service.
It should be designed as a structured layer of care delivery.
The goal is to connect:
The patient
The treatment pathway
The HCP
The support team
The digital communication channels
The relevant data points
When implemented correctly, this approach can help:
Improve adherence and persistence
Support better treatment outcomes
Identify at-risk patients earlier
Improve patient experience
Reduce unnecessary manual follow-up
Support more scalable chronic care programs
Reduce administrative burden on clinical teams
Conclusion
The future of chronic care is not only more visits.
It is smarter care between visits.
Digital patient engagement and treatment orchestration can help bridge the gap between the clinic and the patient’s daily life — supporting adherence, persistence, and better care continuity while helping HCPs focus their time where it matters most.
At B-online, we believe that effective chronic care requires connected digital pathways that support patients at home, help providers identify risk earlier, and enable more scalable patient engagement programs across therapeutic areas.




